It's time to stop looking at just the teeth and start looking at the joint, the muscles, and the skeleton for a real cure.
If you have been suffering from jaw pain, clicking, or locking, you may have been told it's because you grind your teeth. You might have been given a night guard and sent on your way. But what if the pain didn't stop?
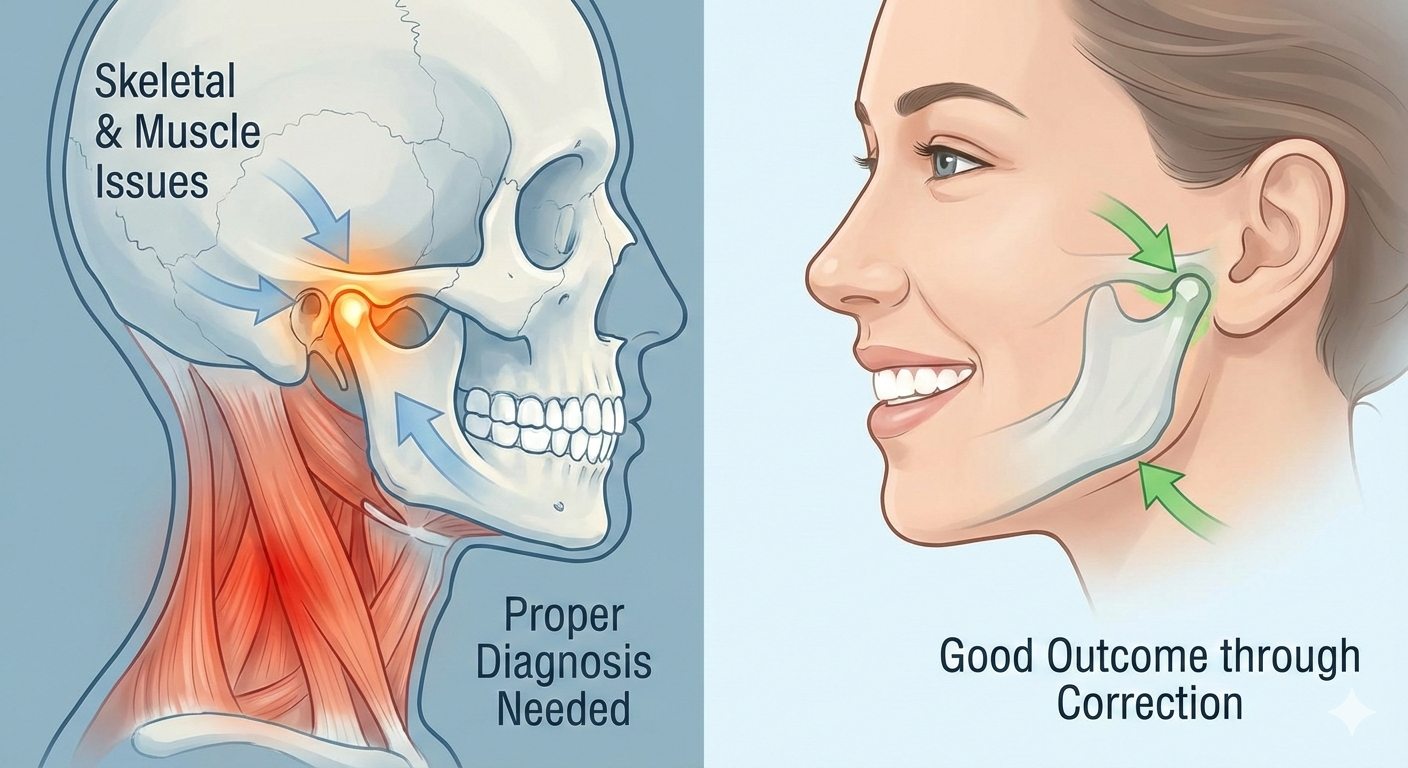
The reality is that Temporomandibular Joint Disorder (TMJ/TMD) is frequently misdiagnosed as purely a dental issue. For many patients, the root cause lies deep within the skeletal alignment of the jaw or the neuromuscular balance of the head and neck.
This guide explores why "perfect teeth" can still mean a painful jaw, and how proper diagnosis leads to skeletal and muscular corrections that finally work.
1. The Myth: "It's All About Your Bite"
For decades, the standard approach to jaw pain was simple: fix the bite, fix the pain. While dental occlusion (how your teeth fit together) plays a role, it is often a symptom rather than the cause.
The Non-Dental Reality:
- Muscular Dysfunction: Chronic muscle tension in the masseter (chewing muscle) and temporalis (temple muscle) can pull the jaw out of alignment, regardless of tooth position.
- Skeletal Discrepancies: If your lower jaw (mandible) is structurally smaller or positioned further back than your upper jaw (maxilla), the joint is constantly strained.
- Postural Influence: "Forward head posture" forces the lower jaw backward, compressing the TMJ joint space and pinching the sensitive retrodiscal tissues.
Key Takeaway:
You can have straight teeth and a perfect smile, but still suffer from debilitating TMJ pain if the underlying skeletal and muscular framework is dysfunctional.
2. Muscular vs. Skeletal TMJ: Understanding the Difference
To achieve a good outcome, you must first identify which type of TMJ issue you are fighting.
Muscular TMJ (Myofascial Pain)
This is often stress-induced or posture-related. The muscles are overworked and in spasm.
Symptoms: Dull aching facial pain, tight neck, headaches (temples), and fatigue when chewing.
The Correction: This rarely requires drilling teeth. Instead, it requires neuromuscular therapy, physical therapy, trigger point injections, or TENS (Transcutaneous Electrical Nerve Stimulation) to relax the muscles and "reset" the jaw's resting position.
Skeletal TMJ (Joint Pathology)
This involves the hard and soft tissues inside the joint itself.
Symptoms: Sharp pain, "crunching" sounds (crepitus), localized joint swelling, or an "open bite" developing where teeth no longer touch.
The Correction: Treatment focuses on decompressing the joint. This might involve orthopedic appliances (splints) that act like "crutches" for the jaw to let the joint heal, or in some cases, orthodontic expansion or surgery to correct the bone alignment.
3. The Critical Step: Proper Diagnosis
The biggest barrier to a good outcome is a generic diagnosis. A 5-minute checkup is rarely enough. To differentiate between a tooth problem, a muscle problem, or a skeletal problem, you need:
- CBCT (Cone Beam Computed Tomography): A 3D X-ray that shows the exact position of the condyle (jaw joint) within the socket. Is the bone deteriorating? Is the joint space compressed?
- MRI (Magnetic Resonance Imaging): Essential for seeing the articular disc. Many patients have a "displaced disc" that X-rays cannot see.
- Joint Vibration Analysis (JVA): Measures the friction and vibration of the joint to detect tears or internal derangements.
Common Questions on TMJ Diagnosis
Q: Can a night guard fix skeletal TMJ?
A: Usually, no. A standard night guard protects teeth from grinding, but it does not account for the position of the jaw joint. In some skeletal cases, a generic guard can actually make the joint compression worse.
Q: Why do I have ear pain if it's a jaw issue?
A: The TMJ is located millimeters from the ear canal. Inflammation in the joint or skeletal compression can push against the ear structures, causing ringing (tinnitus), congestion, or earaches.
4. The Path to a Good Outcome
A "good outcome" is defined as a stable joint, a pain-free range of motion, and a bite that supports the joint position.
Phase 1: Skeletal and Muscle Correction
Before moving teeth, we must stabilize the foundation.
- Splint Therapy: Using a specialized orthotic to reposition the lower jaw forward or downward, creating space for the disc to heal and muscles to relax.
- Physiotherapy: Manual therapy to release the pterygoid muscles (deep jaw muscles) that are often inaccessible to self-massage.
Phase 2: Stabilization
Once the pain is gone and the jaw is in a healthy skeletal position, only then do we look at the teeth.
If the new, healthy jaw position means the teeth don't touch correctly, orthodontics or restorative work might be used to build the teeth up to meet the healthy joint position—not the other way around.
Summary
TMJ is a complex interplay of bone, muscle, and nerve. Treating it requires looking beyond the teeth. If you have tried dental treatments without success, it is likely because the skeletal or muscular component was ignored.
The Formula for Relief:
- Proper Diagnosis: 3D Imaging & Joint Analysis
- Skeletal/Muscle Correction: Orthotics & Therapy
- Good Outcome: Pain-free function & Stability
Struggling with Jaw Pain?
Our experienced team at Dr. Dev's Dental Hospital uses advanced diagnostic technology to identify the true cause of your TMJ symptoms. Schedule a comprehensive evaluation today.
Book Your TMJ Consultation